I have recently had discussions with some of my colleagues in regards to the “true” definition of a dedicated device. Something that has been up in the air recently is the way that we are defining these AAC systems (i.e., Speech Generating Devices/SGD). Why is it even important? Well, insurance, for one!
AAC Recap
Augmentative and alternative communication (AAC) is a way to enhance one’s communication, i.e., augment, as well as serve as an alternative means of communication: the back and forth exchange of messages.
AAC comes in many forms: no tech, low tech, mid tech, and high tech. High tech AAC involves the use of an electronic device with auditory output that contains more advanced processors (as compared to mid tech AAC). This type of device is commonly referred to as a speech-generating device.
Speech-generating devices can be expensive, though there are many funding options available. Some individuals who use high tech AAC have a "dedicated" device, which means they only use this device for communication. Other individuals who use high tech AAC have devices that they use for both communication and other purposes. We break down the key differences below!
Looking for AAC Goals?
Check out our AAC Master Goal Bank, which contains thousands of goal possibilities for children and adults.
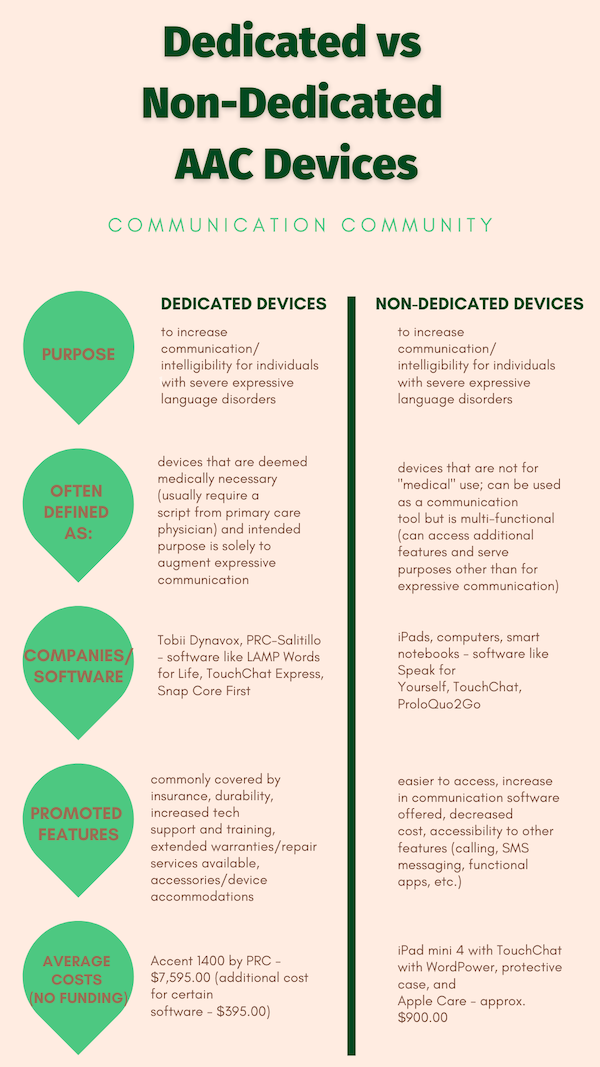
Dedicated vs Non-Dedicated Devices
Oftentimes, dedicated devices are more likely to be covered by private insurance, Medicare, and Medicaid as opposed to non-dedicated devices. If you are a client or caregiver interested in applying for funding for an SGD, it seems like a dedicated device is the way to go, right? Maybe. Maybe not. An increase in new communication software on the market (think: speech-generating applications on an iPad - aka non-dedicated device) has changed client and caregiver accessibility to augmentative communication. The “defining” piece is important because insurance policies that only report dedicated devices as considered/approved for funding can make an enormous difference in the options we provide to clients.
For those of you who are newer to the AAC game, therapists tend to think of SGDs in two different categories: dedicated devices and non-dedicated devices. Again, the way that we define each subcategory of SGDs tends to vary slightly depending on who you ask - there is variability across insurance carriers and policies state by state. For example, in the state of Massachusetts, MassHealth will consider funding for non-dedicated devices; however, there is only “limited” coverage under “certain circumstances.”
How do these devices differ?
As you could probably notice, there are definitely pros and cons for each type of device. One of the largest is the gap in cost. Though, most of the time, if the client/caregiver applying for funding is in great need of the device and has clinical evidence to support its need, the individual should not have a problem obtaining a funded dedicated device.
It should be noted that turnaround time is something to consider. It can take several months, lengthy paperwork, and support from a certified speech-language pathologist (usually a comprehensive AAC evaluation) by the time you receive your device.
Yes, you could technically buy, download, and put together a completed non-dedicated device in one day (excluding time to edit layouts/vocabulary), but that is still just under a grand coming out of someone's pocket. Either way, it is important to know and understand your options.
Looking for more AAC resources?
Check out some of our top posts related to dedicated and non-dedicated devices:
- How to Make a Communication Board
- What is Aided Language Stimulation?
- Access Options for AAC
- How to Optimize AAC Devices
- Why You Should Back up AAC Devices
- AAC Device Accessories
Citations/further resources:
https://leader.pubs.asha.org/doi/full/10.1044/leader.BML.19052014.26