Dysphagia, also known as difficulty swallowing, may be caused by many disorders or impairments, and can affect children or adults, though it affects adults more. In this post, we will focus on dysphagia in the adult population. Someone who has dysphagia is typically affected by other medical conditions, including neurological or physical issues. Individuals who have dysphagia may be evaluated and treated by a speech-language pathologist (SLP).
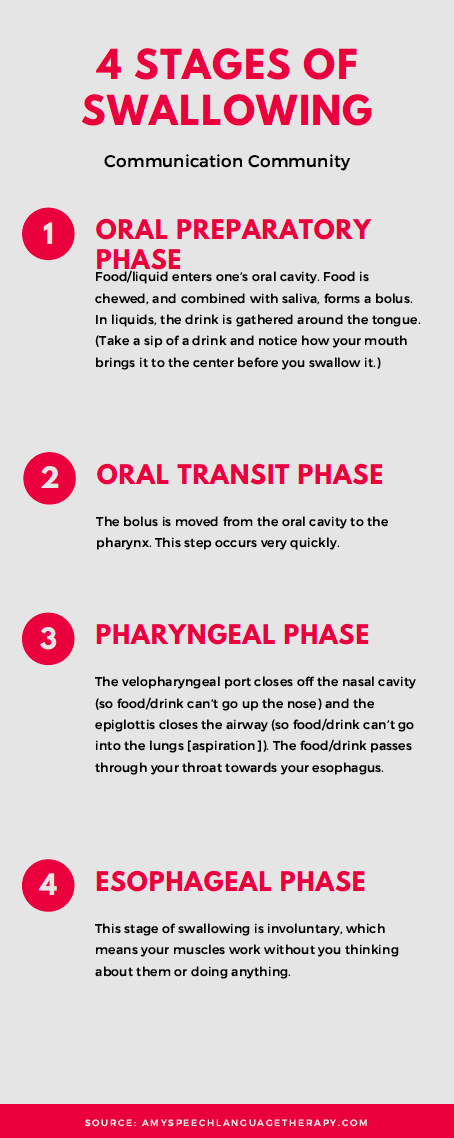
The Four Stages of Swallowing
Though most of us do not actively think about swallowing when we are eating or drinking something, it is actually a complex process involving many muscles and precise timing. Before food or drink ends up in one’s stomach, first it must pass through their oral cavity, pharynx and esophagus. Difficulty moving food or drink through one’s oral cavity (mouth), pharynx (throat), and esophagus is classified as dysphagia. Many muscles work together to ensure food is chewed properly and sent back to the throat and down the esophagus. The airway to the lungs are temporarily closed off when you swallow to ensure food/drink doesn’t go into them. If they do, this is called aspiration (you know, like when something “goes down the wrong pipe”). Aspirating and choking are often used synonymously. However, aspiration can also be sneaky, so you may hear a clinical term called “silent aspiration.” Silent aspiration is when there aren’t really any of those overt signs of choking (think: coughing or apparent breathing difficulties). This can be a precursor for individuals who develop aspiration pneumonia.
In summary, when the muscles don’t work together properly due to neurological or physical conditions, difficulty swallowing may occur. SLPs typically work with individuals with dysphagia due to problems within their oral cavity and pharynx.
Symptoms of Adult Dysphagia
According to ASHA, symptoms of dysphagia include:
- Drooling/food secretions
- Food remaining in mouth
- Food/liquid leaking from nasal cavity (nose)
- Feeling of fullness in throat
- Pain when swallowing
- Voice sounds wet/gurgly after swallowing
- Difficulty breathing when eating/drinking
- Extra time needed to eat/drink
- Avoiding certain foods/drinks
- Physical changes - dehydration, unintentional weight loss
- Recurring pneumonia or respiratory infections
Symptoms of dysphagia may be very obvious - e.g. an individual coughs excessively after eating or drinking, or some food or liquid is left in their mouth after swallowing. However, some symptoms may not be obvious - some liquid may go into one’s lungs instead of down their throat, but it doesn’t cause them to cough excessively after (remember silent aspiration?). Additionally, it is normal that you may sometimes cough after swallowing something or start laughing while drinking and the liquid goes up your nose. However, if it is more than a once in a while occurrence (paired with weakness or paralysis in the muscles in the mouth/throat), it may be a symptom of dysphagia.
Causes of Adult Dysphagia
As mentioned previously, neurological or physical impairments may cause an individual to have dysphagia. More specifically, dysphagia in adults may be due to stroke, brain injury, degenerative disease (e.g. ALS), dementia, Parkinson’s disease, developmental disabilities (e.g. cerebral palsy), cancer (in the mouth/throat area), trauma (in the mouth/throat area), infectious diseases, or pulmonary diseases. Not ALL individuals who have a stroke or infectious disease will have dysphagia, but some will.
Adult Dysphagia Evaluations
Dysphagia evaluations, like all evaluations, include reviewing an individual’s case history and prior medical history. Specific to dysphagia evaluations are non-instrumental and instrumental assessment practices. It is common that a dysphagia evaluation includes both non-instrumental and instrumental assessments.
Non-Instrumental Evaluations:
The SLP will likely do an oral mechanism exam, which includes looking inside one’s mouth and checking out the tongue, teeth, hard palate, and more. They will consider the structure of them (e.g. is the hard palate fully intact?), as well as the function (e.g. can the tongue move well?). Depending on the status of the oral mechanism exam, they may give the individual ice chips, or small amounts of food or liquid, and observe how an individual swallows them. The SLP will likely be looking out for any of the symptoms mentioned above (e.g. drooling or coughing after swallowing). They may see if/how an individual’s swallow changes if using a spoon or a straw when drinking. If they do notice symptoms of dysphagia, they may also test out different treatment options during the evaluation as well.
Instrumental Evaluations
Individuals who are being evaluated for dysphagia may undergo a Modified Barium Swallow (MBS) test or a Fiberoptic Endoscopic Evaluation of Swallowing (FEES) procedure. During a MBS test, an individual is given foods/liquids, and are observed via a fluoroscopy, which is a type of X-Ray. SLPs who are trained in assessing dysphagia via MBS tests can observe whether or not food and liquid is aspirated, or goes into one’s lungs.
This video shows an example of a MBS test.
During a FEES procedure, a (very small and thin) instrument with a small camera and light on the end is inserted into one’s nose, and passes through so the camera rests above the epiglottis. Here, the SLP can see the structure of the throat which may not be visible through the mouth. An individual swallows saliva, and/or is given a food/drink and observed via the camera to see how the muscles/structures work when swallowing.
This video shows an example of a FEES test.
There are pros and cons to each of the instrumental exams; what is best for one person may not be ideal for another. Consulting with an SLP or medical professional is always advised!
Treatment Options for Dysphagia
There are many different treatment options and modifications for dysphagia. This may include thickening liquids so that they are easier to swallow, avoiding foods that are difficult to swallow, and compensatory strategies such as taking deliberately small bites of food or drinks. All treatment options should be considered carefully depending on the individual and their medical history, background, and abilities - there is no one-size-fits-all treatment strategy!
Liquids may be thickened to various degrees. Thin, or regular liquid is unthickened, followed by nectar (thick), honey (thicker), and pudding (thickest). Specific thickening agents are available for purchase if it is advised an individual thickens liquids due to dysphagia.
Solids may be altered to make them easier to swallow. This may include cutting food into small pieces, only eating soft foods (e.g. pasta over steak), or only eating pureed foods.
Compensatory strategies may include taking small bites of food and drinks, eating more slowly, turning the head to one side when swallowing, or coughing after swallowing to ensure no food/liquid enters the airway. Other strategies may be not using a straw when drinking.
Conclusions
As with all disorders or impairments related to the field of speech-language pathology, it is best to consult with an SLP and medical professional for assessments and evaluations if you have concerns about difficulty swallowing. Below are more sources about the symptoms, causes, evaluations, and treatment options for dysphagia.
Citations/Further resources:
https://www.amyspeechlanguagetherapy.com/the-normal-swallowing-process.html